
The hardships of being poor include killing you
Sounds sensational but it's true and living in a western 'developed' nation is not protective

“….social injustice is killing people on a grand scale” — Mikonnen & Raphael; Social Determinants of Health: The Canadian Facts, 2010
Non-communicable diseases (NCDs), also referred to as chronic diseases, are diseases that aren’t transmissible from one person to another but are estimated to account for 74% of all deaths globally (NCDs and Health). Of all chronic disease deaths, 77% occur in low- and middle-income countries, and that becomes even worse when death occurs prematurely (defined as prior to 70 years of age), where 86% of those deaths occur in low- and middle-income countries.
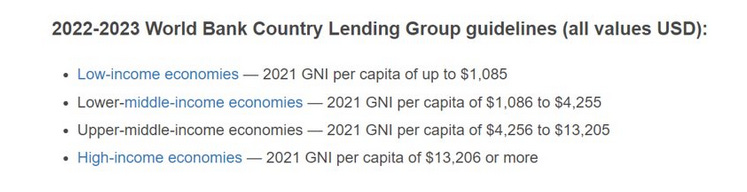
The world bank defines low and middle-income economies using gross national income (GNI; in US dollars) as above.
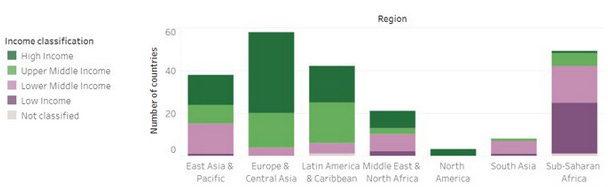
It’s not surprising to see where the low-income and middle-income countries reside in our world (New World Bank country classifications 2022-23). Urbanization of these countries and with that the increased prevalence of risk factors such as smoking, alcohol consumption, poor diet and inactivity, contributes to increased chronic disease deaths but cannot fully account for the higher levels.
While income in North America is considered to be ‘high’ there are plenty of people living under the poverty line. In my own country, Canada, low income cut-offs after tax are based on whether someone lives rurally or in a city of a certain size Poverty lines in Canada. So, a family of 4 living in a rural area, for example, was considered in 2021 to be in poverty if the income was below $28200 while a family of 4 living in a large city would be in poverty if income was below $43110.
So, does it really matter for a society like Canada if there are low-income families? If there are families with children that struggle to make ends meet consistently, with less food on the table, less secure housing, etc.? Well, if you look at it purely from the perspective of the health of those families, yes, it does matter. It matters a lot.
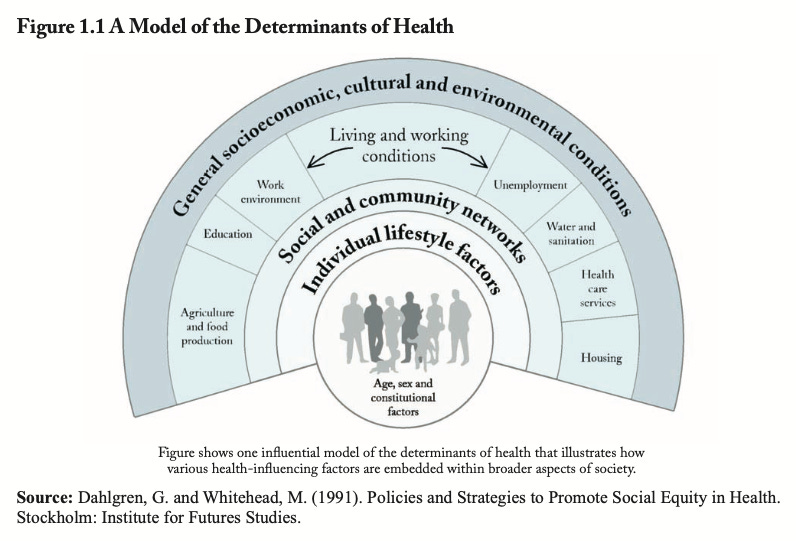
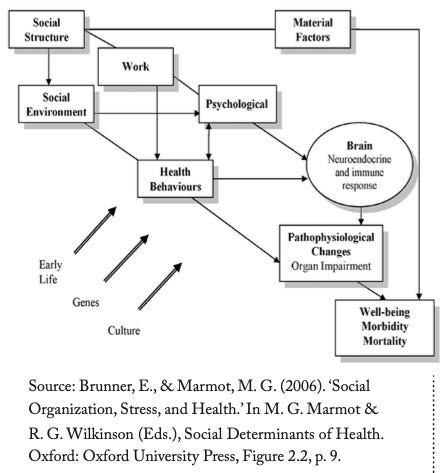
The model above brings many factors to bear on the determinants of health and thus the related incidence of chronic disease. These go well beyond constitutional factors (e.g., genetic factors) and lifestyle choices. If you focus on the outer three rings, you will see many factors associated with socioeconomic status and poverty. Lower education, unemployment, substandard housing, less access to health care services among others, have been shown to negatively influence health in many people.
In other words, these factors will lead to some in society inevitably faring better than others with respect to health - termed ‘health inequity’. How long you live and whether you end up with chronic diseases, such as heart disease and obesity, are directly influenced by these social factors and tend to be unequal among the inhabitants of nations, such as Canada, that call themselves ‘developed’. The following is a direct quote from the original 2010 edition: Social Determinants of Health: The Canadian Facts
We have known for a very long time that health inequities exist. These inequities affect all Canadians but they have especially strong impacts upon the health of those living in poverty. Adding social sciences evidence – the understanding of social structures and of power relationships – we have now accumulated indisputable evidence that “social injustice is killing people on a grand scale.” (original italics)
The second edition, published in 2020, brings numbers up to date but does not have anything more rosy to say with respect to income disparity. Canada is now above the OECD average for income inequality, slightly better than in 2010:
As a result of these trends, from 1980 to 2015, the bottom 60 percent of Canadian families experienced very small increases in market incomes in constant dollars while the top 20 percent of Canadian families did very well. After taxes and government transfers, this picture improves somewhat with slight increases for the bottom 60 percent of Canadians, but these increases are dwarfed by the increases experienced by the wealthiest 20 percent of Canadians.
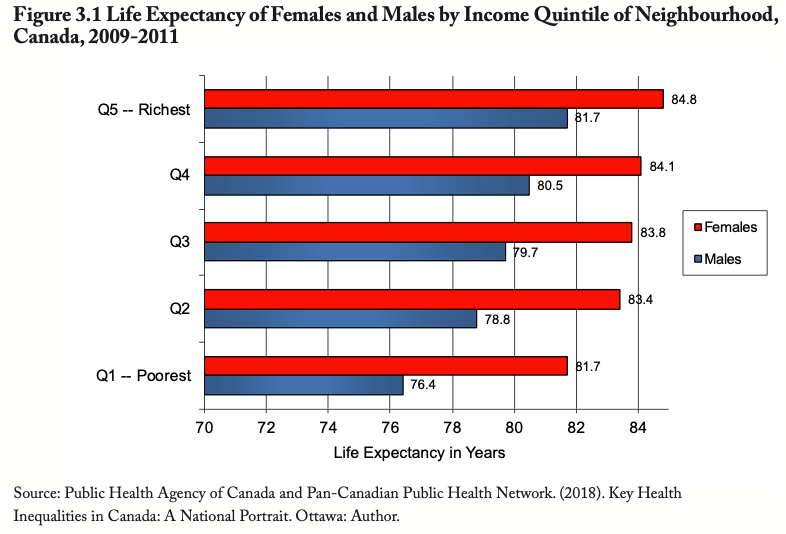
As is easily seen in the above figure from the 2020 report, the poorest Canadian males die on average more than 5 years earlier than the richest Canadian males, while the discrepancy in poor and rich Canadian females is closer to 3 years. But death is only one health outcome (the final one) and let’s face it, it’s important, but so is living with health (or not).
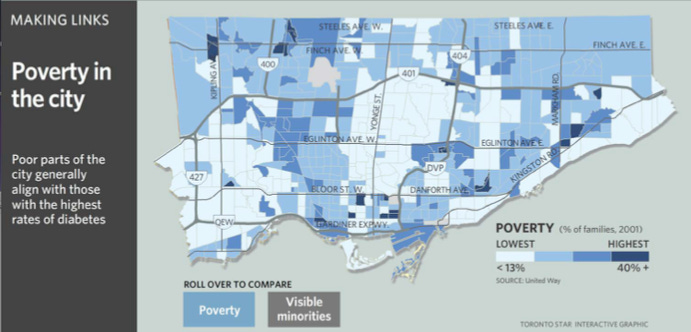
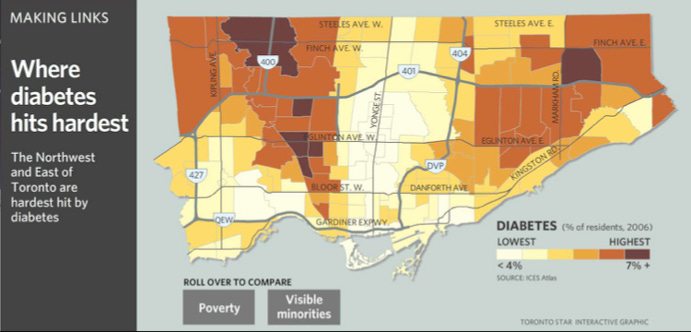
Chronic, non-communicable diseases such as diabetes and heart disease exact a heavy toll on those afflicted, many of whom reside in the poorest neighbourhoods of our major cities. Monsebraaten, L. and Daly, R. (November 1, 2007). Diabetes Lurks in Urban Sprawl. This report isn’t recent, but nothing has changed. In fact, we know from the pandemic that lower income persons were hit the worst with respect to infection rates, hospitalizations (CBC News (2020). Lower income people, new immigrants at higher COVID-19 risk in Toronto) and loss of income as a result of lockdowns.
Diabetes and health disease, among other chronic but preventable diseases, often share a common underlying physiological mechanism - that of repeated and persistent exposure to stressful experiences. For a primer on the stress response, see a prior post (https://taraperrot.substack.com/p/get-a-grip-intro-a-primer-on-handling). When we talk about repeated and/or persistent exposure to stressful events, we are talking about damaging events that occur in the body and brain.
Food and housing insecurities, joblessness or precarious employment, and other aspects of low-income families result in repeated and/or persistent release of the major stress hormone, cortisol. Cortisol’s job in the body during an adaptive stress response is catabolic - it breaks down things for use as energy and therefore is meant to be released temporarily and infrequently. Cortisol acts on various parts of the brain and when released frequently and in excess, actually kills brain cells, affecting behaviour, well-being, mental health, memory. The same occurs in other organs such as the kidney, liver, blood vessels, and heart. The immune system is also shut down by stress hormones when they are released in excess (see review of the effects of cortisol on the body).
While providing only a temporary reprieve, those suffering from the effects of repeated and/or persistent release of cortisol often resort to unhealthy behaviours to cope, at least in the short-term - tobacco, alcohol, and other substance abuse, over-eating. Unfortunately, these behaviours in the long term perpetuate the potential for diseases.
The 2020 report has many recommendations for the government. The authors had many of the same recommendations in their report of 2010. Times certainly aren’t any easier now so it’s difficult to envision the Canadian government enacting any of the recommendations and as a result, low-income Canadians will continue to be at risk of suffering from ill-health and as a result to make more use of a health care system that is in critical condition.
Finally, in many poor families there are poor children. There were poor mothers gestating those children. The impact of poverty on programming the brain and body during early life will have to wait for another post, but I hope you will join me for that important discussion.
Thanks for reading and as always, I welcome your thoughts.
‘Food and housing insecurities, joblessness or precarious employment, and other aspects of low-income families result in repeated and/or persistent release of the major stress hormone, cortisol….’
Yeah, it’s all linked, and reveals just how damaging wealth inequality is to society.
Wealth inequality should be considered a top concern for countries in general and must be addressed immediately.